- Enter the current measured serum Na⁺ (mEq/L), body weight, and the total-body-water fraction (sex/age) — these set total body water.
- Enter the time interval (hours) over which the sources are given, and set duration (chronic vs. acute) and any high-ODS risk factors (alcoholism, malnutrition, K⁺ < 3.0, liver disease) — these set the safe ceiling (6 / 8 / 12 mEq/L per 24 h).
- Add up to three sodium sources in any combination — IV saline (3% / 2% / 1.5% / NS) and/or oral NaCl / NaHCO₃ tablets — each with its dose (mL for fluids, number of tablets for oral). Leave unused slots on “— none —”.
- Read the live result: the combined ΔNa⁺ from all sources, predicted serum Na⁺, the correction rate, and the projected 24-h rise versus the safe ceiling (green = within, red = exceeds).
- Treat the ceiling as a hard limit — if exceeded, reduce a source, slow the rate, or extend the interval, and recheck Na⁺ every 2–4 h.
All computation runs in your browser; no values are stored or transmitted.
When to Use
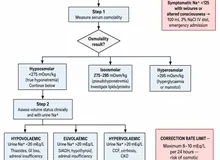
Use this tool when managing a patient with hyponatremia (serum Na⁺ < 135 mEq/L) who requires active sodium correction. It computes the maximum safe correction targets at 24 and 48 hours to prevent osmotic demyelination syndrome (ODS), formerly called central pontine myelinolysis.
Appropriate use
Any patient with symptomatic or asymptomatic hyponatremia of chronic or uncertain duration who needs planned sodium correction, whether via fluid restriction, isotonic saline, hypertonic saline (3% NaCl), or treatment of the underlying cause (SIADH, hypothyroidism, adrenal insufficiency). Most critical in patients with Na⁺ < 125 mEq/L, those on hypotonic fluids post-operatively, or those with SIADH.
When NOT to rely on it alone
In acute symptomatic hyponatremia (seizures, respiratory arrest, coma) with onset clearly within 48 hours, faster initial correction of +4–6 mEq/L in the first hour using 3% NaCl 150 mL IV is appropriate regardless of this calculator's output. Do not use this calculator to authorize correction faster than 10 mEq/L per 24 hours without direct expert guidance.
Pearls & Pitfalls
When in doubt, treat as chronic
Duration is often uncertain in outpatient or community presentations. Treating an acute hyponatremia as chronic means a slightly slower correction — a small trade-off for avoiding catastrophic ODS. The consequences of over-correction are irreversible; the consequences of slower correction are almost always manageable.
Monitor sodium frequently during active correction
Check serum sodium every 2–4 hours during any active correction strategy, especially when using hypertonic saline or when a patient unexpectedly reverses SIADH (e.g., after stopping a causative drug or treating pain). Auto-correction is a real risk — the patient's own kidneys may excrete dilute urine faster than expected once the precipitant resolves, causing the sodium to rise without any infusion change.
Pitfalls
(1) Never use this calculator to justify rapid correction "because the duration is uncertain" — when uncertain, always choose the chronic path. (2) Hypokalemia potentiates ODS independently — correct potassium concurrently; potassium infusion itself raises serum sodium via the Gibbs–Donnan effect (1 mEq K⁺ replaces ~1 mEq of Na⁺ shift). (3) If sodium rises faster than planned, do not wait for the next check — act immediately with DDAVP and free water. (4) This calculator does not compute infusion rates or the Adrogue–Madias formula for predicting the effect of a specific fluid; it computes ceilings only.
Why Use It
Overcorrection of chronic hyponatremia is one of the most feared iatrogenic neurological injuries in hospital medicine. When serum sodium has been chronically low, brain cells compensate by losing organic osmolytes over 24–48 hours. Rapid re-elevation of serum sodium pulls water out of those cells faster than they can replenish osmolytes, causing osmotic demyelination — a demyelinating injury affecting the pons and extrapontine sites that produces dysarthria, dysphagia, paraparesis, and the locked-in syndrome. ODS is largely irreversible. The threshold of harm is correction exceeding 10–12 mEq/L in 24 hours in the general population and 6 mEq/L in 24 hours in the highest-risk group (alcohol use disorder, malnutrition, hypokalemia, liver disease, or baseline Na⁺ < 105 mEq/L).
Conversely, under-correction of acute symptomatic hyponatremia leaves the patient at risk of cerebral edema, herniation, and death. This calculator navigates both failure modes by stratifying risk and providing concrete target numbers.
Hyponatremia Correction — Rate & Sodium-Rise Predictor
Enter the patient's sodium and weight, then add up to three sodium sources — IV saline (3% / 2% / 1.5% / NS) and/or oral NaCl / NaHCO₃ tablets, in any combination. The tool sums them and predicts the total rise in serum Na⁺, the correction rate, and whether the plan stays within the ODS-safe ceiling.
Pick a source and its dose for each slot. Leave a slot on “— none —” if unused.
⚕ Combined ΔNa = (Σ Na delivered − Serum Na × Σ infused volume) ÷ (TBW + Σ infused volume); TBW = weight × fraction. Oral tablets add Na with ~no volume; IV fluids add both. Correction targets are CEILINGS, not goals — monitor Na⁺ every 2–4 h. If overcorrection occurs, give desmopressin (DDAVP) 1–2 mcg IV/SC. Hypertonic (2–3%) saline requires a monitored / ICU setting. Physician judgement required.
Next Steps
Use the result to support — not replace — clinical judgment.
- Interpret the value against the targets shown in the calculator and the Evidence section below, in the context of the full clinical picture.
- Trend serial measurements rather than acting on a single result; confirm abnormal or unexpected values before changing management.
- Apply the relevant KDIGO / specialty-guideline threshold and document the indication.
- Escalate or refer to nephrology when results are out of range, rapidly changing, or discordant with the clinical picture — and discuss the implications with the patient.
Evidence & References
Formula & Equations
| Condition | Max correction per 24 h | Max correction per 48 h |
|---|---|---|
| Chronic hyponatremia, no high-risk factors | 8–10 mEq/L | 18 mEq/L |
| Chronic hyponatremia, high-risk factors (alcohol, malnutrition, K⁺<3, liver disease, or Na⁺<105) | 6 mEq/L | 12 mEq/L |
| Acute hyponatremia (<48 h, confirmed) | 12 mEq/L (symptom-driven) | 24 mEq/L |
The 24-hour Na⁺ target = min(current Na⁺ + maxPer24, 145). The calculator applies the Na⁺ = 120 threshold: any patient with a starting Na⁺ < 120 mEq/L is automatically escalated to the high-risk tier regardless of other factors, because severely depleted brain osmolytes carry the highest ODS risk.
Emergency acute symptomatic protocol (for reference)
| Step | Action | Target |
|---|---|---|
| Seizing / unconscious | 3% NaCl 150 mL IV over 20 min; repeat ×2 if no improvement | Na⁺ rise of +5 mEq/L in first hour |
| Once symptoms resolve | Stop 3% NaCl; switch to isotonic or restrict fluids | Do not exceed daily limit from this calculator |
| Overcorrection detected | Desmopressin 1–2 mcg IV/SC + 3–5 mL/kg D5W over 1–2 h | Re-lower sodium to below the daily ceiling |
Evidence & References
The correction-rate limits derive from retrospective and prospective case series linking rapid correction to ODS and from the landmark 2014 European clinical practice guideline (Spasovski et al.) and the 2015 NEJM review by Sterns. The Adrogué–Madias 2000 NEJM review remains the standard reference for pathophysiology and management targets. The high-risk 6 mEq/L ceiling is supported by multiple case series showing ODS events at rates below 10 mEq/24 h in patients with alcohol use disorder, malnutrition, and severe hypokalemia.
- Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000;342(21):1581–1589.
- Sterns RH. Disorders of plasma sodium — causes, consequences, and correction. N Engl J Med. 2015;372(1):55–65.
- Spasovski G, Vanholder R, Allolio B, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Eur J Endocrinol. 2014;170(3):G1–G47.
- Sterns RH, Hix JK, Silver SM. Treating profound hyponatremia: a strategy for controlled correction. Am J Kidney Dis. 2010;56(4):774–779.