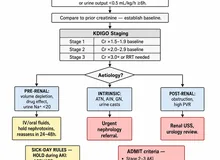
- Confirm the patient has early AKI (KDIGO stage 1–2), is volume-replete (euvolemic), and has no obstruction or ongoing nephrotoxin/hypotension before testing.
- Enter the patient's weight (kg) and select prior loop-diuretic exposure. The recommended IV furosemide dose updates automatically (1.0 mg/kg if loop-naïve, 1.5 mg/kg if prior loop exposure).
- Give the dose as a single standardized IV bolus, then record the urine output over the next 2 hours and enter it (mL).
- A 2-hour urine output ≥ 200 mL = FST responsive ("passed") — lower risk of progression; < 200 mL = FST non-responsive ("failed") — predicts progression to KDIGO stage 3 AKI / need for RRT.
All computation runs in your browser; no values are stored or transmitted.
When to Use
Use the Furosemide Stress Test in a patient with early acute kidney injury (KDIGO stage 1–2) when you need to predict whether the AKI will progress to severe (stage 3) injury or require renal replacement therapy. It is a bedside functional test of tubular reserve: a robust diuretic response to a standardized loop-diuretic bolus signals preserved tubular function and lower risk, while a blunted response (2-hour urine output < 200 mL) predicts progression. In the validation cohorts, a 2-hour output < 200 mL predicted stage-3 progression with roughly 87% sensitivity and 84% specificity, outperforming many novel AKI biomarkers.
Appropriate population
Critically ill or hospitalized adults with established early AKI (KDIGO stage 1–2) who are volume-replete (euvolemic) — ideally tested after adequate volume resuscitation. Particularly valuable in the nephrology–ICU setting for risk-stratifying who may need escalation, monitoring, and timely RRT-access planning.
When NOT to rely on it
Do not use the FST in a hypovolemic patient (a poor response then reflects volume depletion, not tubular failure) — give it only after volume resuscitation. Exclude urinary tract obstruction and ongoing nephrotoxin exposure or hypotension first. It is validated only in early AKI (stage 1–2), not in chronic dialysis-dependent ESKD, and it is not a treatment — it is a one-time diagnostic/prognostic bolus.
Pearls & Pitfalls
200 mL over 2 hours is the threshold
The cut-point is simple: total urine output of ≥ 200 mL in the 2 hours after the bolus = responsive ("passed"), lower risk of progression; < 200 mL = non-responsive ("failed"), which predicts progression to KDIGO stage 3 AKI and the need for RRT. The test reports tubular reserve as a single, actionable yes/no at the bedside.
Standardize the conditions
Give a single standardized IV bolus — 1.0 mg/kg if loop-naïve, 1.5 mg/kg if the patient has had prior loop diuretics. Ensure the patient is euvolemic before testing; a poor response in a hypovolemic patient is uninterpretable. Replace urinary losses (e.g., with isotonic fluid) during and after the test to avoid inducing hypovolemia from the brisk diuresis.
Pitfalls
(1) Validated only in early AKI (stage 1–2) in volume-replete patients — not in hypovolemia, established stage-3 AKI, or chronic ESKD. (2) Exclude urinary obstruction first (check the catheter/bladder) — a blocked drain mimics a failed test. (3) Ongoing nephrotoxins or hypotension bias the result and should be corrected. (4) It is a prognostic bolus, not therapy — a "passed" FST does not mean the AKI is resolved, and a "failed" FST is a prompt to optimize hemodynamics, stop nephrotoxins, and plan monitoring/RRT access.
Why Use It
Predicting which patients with early AKI will progress to severe injury or dialysis is one of the hardest calls in the nephrology–ICU. The Furosemide Stress Test answers it with a cheap, fast, bedside functional probe of tubular reserve rather than a static biomarker. A patient who mounts a brisk diuresis (≥ 200 mL over 2 hours) has preserved tubular function and a lower risk of progression; one who cannot (< 200 mL) is flagged early — before serum creatinine fully declares — so the team can optimize hemodynamics, withdraw nephrotoxins, and plan monitoring and RRT access proactively. In head-to-head validation, the FST outperformed several novel AKI biomarkers for predicting progression to KDIGO stage 3, which is why it has become a practical, widely cited risk-stratification tool in critical-care nephrology.
Furosemide Stress Test (FST)
Enter the patient's weight and prior loop-diuretic exposure to get the recommended standardized IV furosemide dose. After giving the bolus, enter the 2-hour urine output for the FST result (responsive ≥ 200 mL vs. non-responsive < 200 mL).
⚕ Chawla LS, et al. Crit Care. 2013;17(5):R207; Koyner JL, et al. J Am Soc Nephrol. 2015;26(8):2023–2031. The FST is validated only in early AKI (KDIGO stage 1–2) in volume-replete patients. Ensure euvolemia, exclude obstruction, and correct nephrotoxins/hypotension before testing; replace urinary losses. For licensed clinicians; not a substitute for individualized assessment.
Next Steps
Use the FST result to risk-stratify and direct the next move.
- Responsive (2-h UO ≥ 200 mL): preserved tubular reserve and lower risk of progression. Continue to treat the underlying cause, avoid nephrotoxins, and monitor — a passed FST is reassuring but not proof of resolution.
- Non-responsive (2-h UO < 200 mL): predicts progression to severe (KDIGO stage 3) AKI and likely need for renal replacement therapy. Anticipate severe AKI: optimize hemodynamics, stop nephrotoxins, and plan close monitoring and RRT access early.
- Confirm the patient was euvolemic and obstruction was excluded before acting on a failed test; replace urinary losses to avoid inducing hypovolemia.
- Pair the FST with KDIGO AKI staging and urinary indices such as FENa / FEUrea for the full picture.
Evidence & References
Protocol
| Quantity | Value |
|---|---|
| Dose — loop-naïve | 1.0 mg/kg furosemide IV bolus |
| Dose — prior loop diuretic | 1.5 mg/kg furosemide IV bolus |
| Observation window | Urine output over the next 2 hours |
| 2-h urine output rate | Entered 2-h UO ÷ 2 (mL/hr) |
| Responsiveness threshold | 2-h UO ≥ 200 mL = responsive; < 200 mL = non-responsive |
Interpretation of the 2-hour Urine Output
| 2-h urine output | Interpretation |
|---|---|
| ≥ 200 mL (responsive / "passed") | Preserved tubular reserve — lower risk of progression |
| < 200 mL (non-responsive / "failed") | Predicts progression to KDIGO stage 3 AKI / need for RRT (~87% sensitivity, ~84% specificity) |
Chawla and colleagues developed and standardized the FST, and Koyner and colleagues showed it outperformed several novel biomarkers for predicting AKI severity; a systematic review confirmed its predictive performance for worsening AKI. Validated in early AKI (stage 1–2) in volume-replete patients only.
References
- Chawla LS, Davison DL, Brasha-Mitchell E, et al. Development and standardization of a furosemide stress test to predict the severity of acute kidney injury. Crit Care. 2013;17(5):R207. doi:10.1186/cc13015.
- Koyner JL, Davison DL, Brasha-Mitchell E, et al. Furosemide Stress Test and Biomarkers for the Prediction of AKI Severity. J Am Soc Nephrol. 2015;26(8):2023–2031. doi:10.1681/ASN.2014060535.
- Rewa OG, Bagshaw SM, Wang X, et al. The furosemide stress test for prediction of worsening acute kidney injury: a systematic review. J Crit Care. 2019;52:48–54. doi:10.1016/j.jcrc.2019.03.005.