- Enter the patient's body weight in kg.
- Enter the measured serum HCO₃⁻ from a recent ABG or basic metabolic panel.
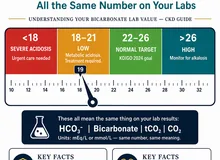
- Enter the target HCO₃⁻ (default 24 mEq/L; for CKD, target 22–24 mEq/L).
- Select the volume-of-distribution factor — use 0.5 for most patients; use 0.7 for severe acidosis (HCO₃⁻ < 10 mEq/L), as Vd increases as bicarbonate falls.
- The result shows total deficit, suggested initial replacement (~½ of deficit), and the equivalent in 50-mEq ampules of 8.4% sodium bicarbonate.
All computation runs in your browser; no values are stored or transmitted. Give initial replacement slowly and recheck ABG/serum HCO₃⁻ before further dosing.
When to Use
Use this calculator to estimate the bicarbonate deficit and guide initial intravenous sodium bicarbonate replacement in adults with metabolic acidosis. The result is a starting estimate — titrate further doses to serial ABG or serum bicarbonate measurements and clinical response.
Appropriate indications for IV bicarbonate
- Severe metabolic acidosis with pH < 7.1 (most experts agree), especially when due to non–anion gap causes (e.g., renal tubular acidosis, diarrhea) or specific toxic ingestions
- Hyperchloremic metabolic acidosis during large-volume normal saline resuscitation
- Acute-on-chronic metabolic acidosis in CKD/ESRD awaiting dialysis
- Bridge therapy in lactic acidosis while treating the underlying cause (controversial — see Pearls)
When NOT to give bicarbonate acutely
Routine IV bicarbonate is not recommended for mild-to-moderate metabolic acidosis (pH > 7.1) in most settings. For CKD metabolic acidosis, use oral alkali therapy (sodium bicarbonate tablets or sodium citrate) rather than IV replacement, targeting a serum HCO₃⁻ of 22–24 mEq/L per KDIGO 2024. Bicarbonate is not indicated as primary therapy for diabetic ketoacidosis (unless pH < 6.9) or for uncomplicated lactic acidosis.
Pearls & Pitfalls
Give only ~½ the calculated deficit initially
Administer approximately half the calculated deficit slowly (e.g., over 4–6 hours as an isotonic NaHCO₃ infusion). Recheck ABG and serum electrolytes before further dosing. The remaining deficit should be guided by repeat measurements and the clinical response, not re-administered blindly.
Critical pitfalls of over-rapid or excessive correction
- Hypernatremia and volume overload: each 50-mEq ampule of 8.4% NaHCO₃ contains ~50 mmol sodium — large doses cause significant sodium and water loading
- Hypokalemia: alkalinization drives K⁺ into cells; check and correct potassium before/during bicarbonate therapy
- Ionized hypocalcemia: alkalosis increases protein binding of calcium, reducing ionized Ca²⁺ — risk of tetany and arrhythmia
- Paradoxical CSF/CNS acidosis: CO₂ produced from bicarbonate buffering crosses the blood-brain barrier faster than HCO₃⁻, transiently worsening CNS acidosis
- Overshoot metabolic alkalosis: particularly with improving renal function or resolution of the underlying cause
CKD-specific guidance
For CKD metabolic acidosis, oral alkali (sodium bicarbonate 650 mg tablets or sodium citrate/citric acid solution) is first-line therapy, not IV bicarbonate. Target serum HCO₃⁻ 22–24 mEq/L per KDIGO 2024 CKD guidelines. Start with 0.5–1 mEq/kg/day orally divided TID and titrate. IV bicarbonate in CKD is reserved for acute severe decompensation or bridge to dialysis.
Treat the underlying cause
Bicarbonate replacement is adjunctive — always identify and treat the primary cause of metabolic acidosis: optimize insulin therapy for DKA, treat sepsis/shock for lactic acidosis, address diarrhea or fistulae for NAGMA, correct renal tubular acidosis, or initiate dialysis for uremic acidosis in ESRD.
Why Use It
Empiric bicarbonate dosing without accounting for body weight and volume of distribution risks both under- and over-correction. Under-correction fails to protect against the hemodynamic consequences of severe acidosis (myocardial depression, vasodilation, arrhythmia); over-correction delivers hazardous sodium loads, precipitates hypokalemia, and can worsen CNS acidosis paradoxically. Quantifying the deficit provides a rational starting dose while preserving the essential next step of serial ABG-guided titration — which this calculator explicitly builds into its output recommendations.
Bicarbonate Deficit & Correction Calculator
Enter body weight, measured serum HCO₃⁻, target HCO₃⁻, and the volume-of-distribution factor to calculate the total deficit and initial replacement dose.
⚕ Formula: HCO₃⁻ deficit (mEq) = Vd × weight (kg) × (target − measured HCO₃⁻). Vd = 0.5 standard; 0.7 for severe acidosis (HCO₃ <10). Give only ~½ the deficit initially and re-titrate to ABG. Each standard 50-mL ampule of 8.4% NaHCO₃ = 50 mEq. Sources: Kraut & Madias 2012; Adrogué & Madias 1998. For clinical use by licensed clinicians only — not a substitute for direct patient assessment.
Next Steps
After calculating and administering the initial dose:
- Give the initial replacement (~½ the total deficit) as an isotonic sodium bicarbonate infusion over 4–6 hours — never as an undiluted bolus unless imminently life-threatening arrhythmia.
- Recheck ABG (or serum HCO₃⁻) and serum electrolytes (Na⁺, K⁺, ionized Ca²⁺) after the initial infusion before administering the remaining deficit.
- Monitor for signs of overcorrection: rising pH >7.50, worsening hypokalemia, tetany, or volume overload.
- For CKD patients: transition to oral alkali (sodium bicarbonate tablets or sodium citrate) once stable, targeting serum HCO₃⁻ 22–24 mEq/L per KDIGO 2024.
- Address the primary cause of metabolic acidosis — bicarbonate is always adjunctive therapy.
- Consult nephrology if pH <7.1, if underlying etiology is unclear, or if the patient has advanced CKD/ESRD requiring dialysis-based correction.
Evidence & References
Formula
| Quantity | Equation |
|---|---|
| HCO₃⁻ deficit (mEq) | Vd × weight (kg) × (target HCO₃⁻ − measured HCO₃⁻) |
| Initial replacement dose | ≈ ½ × total deficit (mEq) |
| NaHCO₃ ampules (8.4%) | total deficit ÷ 50 mEq per ampule |
| Vd (standard) | 0.5 L/kg |
| Vd (severe acidosis, HCO₃ <10) | 0.7 L/kg (Vd increases as HCO₃ falls) |
Worked Example
| Parameter | Value |
|---|---|
| Weight | 70 kg |
| Measured HCO₃⁻ | 14 mEq/L |
| Target HCO₃⁻ | 24 mEq/L |
| Vd factor | 0.5 |
| Total deficit | 0.5 × 70 × (24 − 14) = 350 mEq |
| Initial dose (~½) | ≈ 175 mEq |
| Ampules (50 mEq each) | ~3.5 ampules for initial dose |
KDIGO CKD Oral Alkali Target
For CKD patients with serum HCO₃⁻ persistently <22 mEq/L, KDIGO 2024 recommends oral alkali supplementation targeting HCO₃⁻ 22–24 mEq/L. IV bicarbonate is reserved for acute severe metabolic acidosis or bridge to dialysis. Oral sodium bicarbonate tablets (325 mg = ~4 mEq; 650 mg = ~8 mEq) or sodium citrate/citric acid solution are used; start at 0.5–1 mEq/kg/day divided TID and titrate.
References
- Kraut JA, Madias NE. Treatment of acute metabolic acidosis: a pathophysiologic approach. Nat Rev Nephrol. 2012;8(10):589–601.
- Adrogué HJ, Madias NE. Management of life-threatening acid-base disorders — first of two parts. N Engl J Med. 1998;338(1):26–34.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314.
- Seifter JL. Integration of acid-base and electrolyte disorders. N Engl J Med. 2014;371(19):1821–1831.