| Viral Infections & Vaccinations Guide for CKD · williamriveromd.com |
W.G.M. Rivero MD · FPCP · DPSN · · williamriveromd.com · 2026 |
|
Patient Education · Nephrology
Viral Infections & Vaccinations in CKD
Immune suppression in kidney disease, Philippine vaccine schedule for CKD and dialysis patients, transplant readiness, and household protection strategies.
|
💉
W.G.M. Rivero MD
FPCP · DPSN
Nephrologist
williamriveromd.com
|
3–5× Higher Infection Risk in CKD |
↓Response Vaccine Efficacy in CKD |
Hepatitis B #1 Priority Vaccine |
Annual Flu Vaccine Required |
1Why CKD Impairs Immune Function
Chronic kidney disease causes a state of chronic, low-grade immune dysfunction called uremic immunosuppression. Uremic toxins — substances that accumulate when the kidneys cannot filter the blood — directly impair neutrophil phagocytosis, T-cell proliferation, and B-cell antibody production. The result is a blunted response to both infections and vaccines: seroconversion rates after hepatitis B vaccination drop from >95% in healthy adults to as low as 40–50% in dialysis patients. This is why higher vaccine doses and more frequent boosters are required for CKD patients.
Dialysis patients face additional infection risks beyond immune suppression: vascular access sites (arteriovenous fistulas and central venous catheters) create direct portals for bloodstream infections, and shared dialysis equipment — if not properly sterilized — can transmit blood-borne viruses such as hepatitis B and C. Patients on maintenance immunosuppression after kidney transplantation are at the highest risk of all, susceptible to common, uncommon, and opportunistic infections that would not threaten a healthy person.
2Infection Risk by CKD Stage
| Stage |
eGFR |
Relative Risk |
Key Threats |
| CKD 1–2 | >60 | 1.5–2× | Influenza, pneumococcus |
| CKD 3 | 30–59 | 2–3× | Hepatitis B, influenza, COVID-19 |
| CKD 4–5 (pre-dialysis) | <30 | 3–4× | All above + shingles (zoster) |
| Hemodialysis | on HD | 4–5× | Hepatitis B (blood-borne!), COVID-19, TB |
| Post-transplant | on IS | 5–10× | ALL infections — live vaccines contraindicated |
⚡ Vaccinate Early — Before Dialysis and Before Transplant
CKD patients should not wait until they are sick to think about vaccines. Vaccination BEFORE dialysis and BEFORE transplant is critical — immune response is better at higher eGFR, and live vaccines (MMR, varicella, zoster Zostavax) cannot be given after transplant. Discuss your vaccination status at every CKD 4–5 clinic visit.
| For educational use only. This guide does not replace individualized medical advice from your physician. References: PSMID Immunization Guidelines 2024 · PSN Guidelines · KDIGO 2024 · DOH Philippines vaccine schedule. |
williamriveromd.com
Page 1 of 9 · williamriveromd.com/guides/viral-infections-vaccinations-ckd |
| Viral Infections & Vaccinations Guide for CKD · williamriveromd.com |
W.G.M. Rivero MD · FPCP · DPSN · williamriveromd.com · 2026 |
Vaccine Seroconversion Rates Decline as CKD Progresses
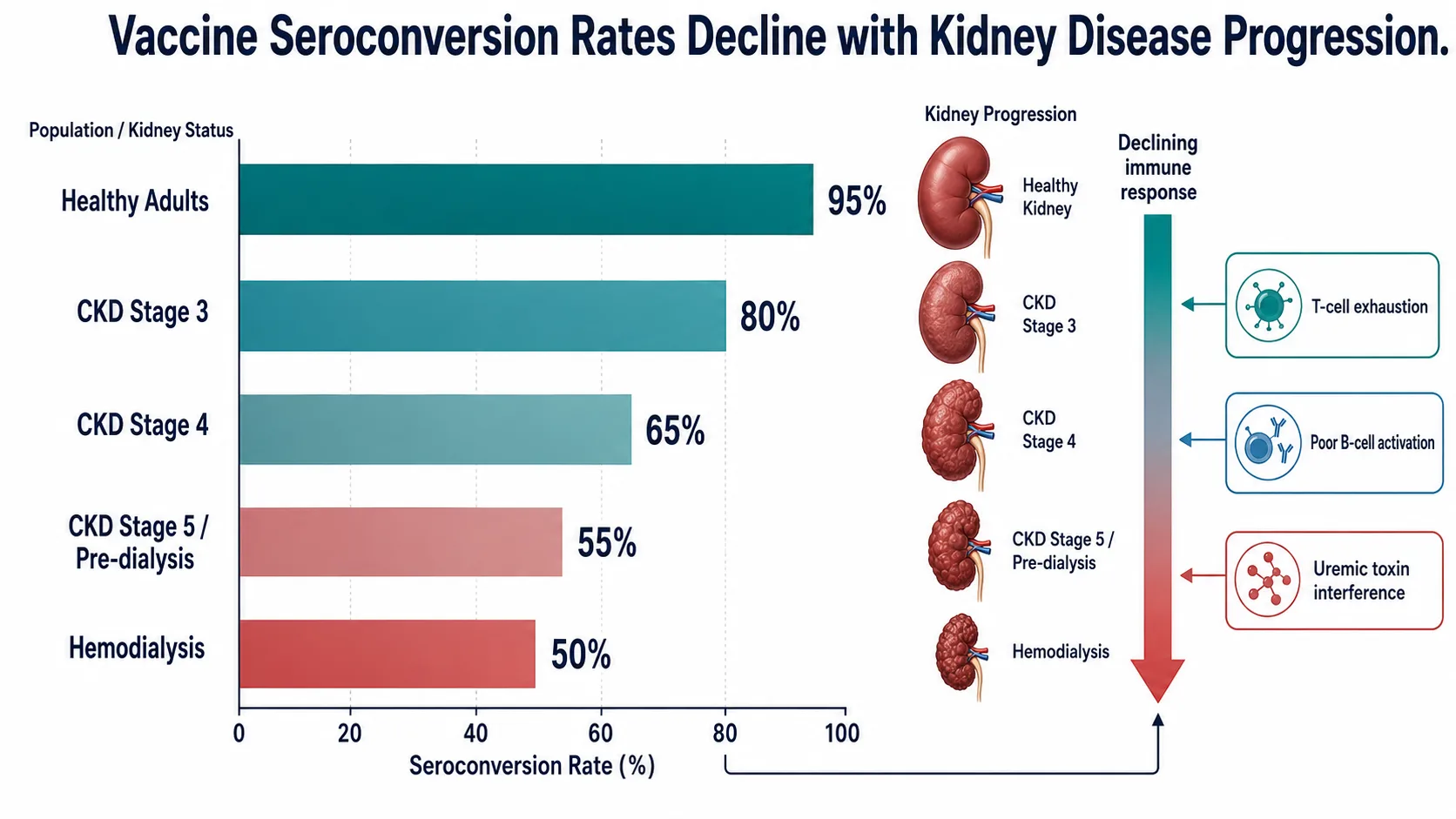
Fig. 1 — Vaccine seroconversion rates decline as CKD progresses. A standard hepatitis B vaccine dose achieves >95% seroconversion in healthy adults, but only 50–60% in CKD stage 4–5, and as low as 40–50% in dialysis patients. Higher doses and more frequent boosters are required. This same immune blunting affects responses to influenza, pneumococcal, and COVID-19 vaccines — making early vaccination (while eGFR is still higher) the most important strategy.
| For educational use only · Not a substitute for individualized medical advice · williamriveromd.com |
williamriveromd.com
Page 2 |
| Viral Infections & Vaccinations Guide for CKD · williamriveromd.com |
W.G.M. Rivero MD · FPCP · DPSN · williamriveromd.com · 2026 |
Live vs Non-Live Vaccines — Safety in CKD
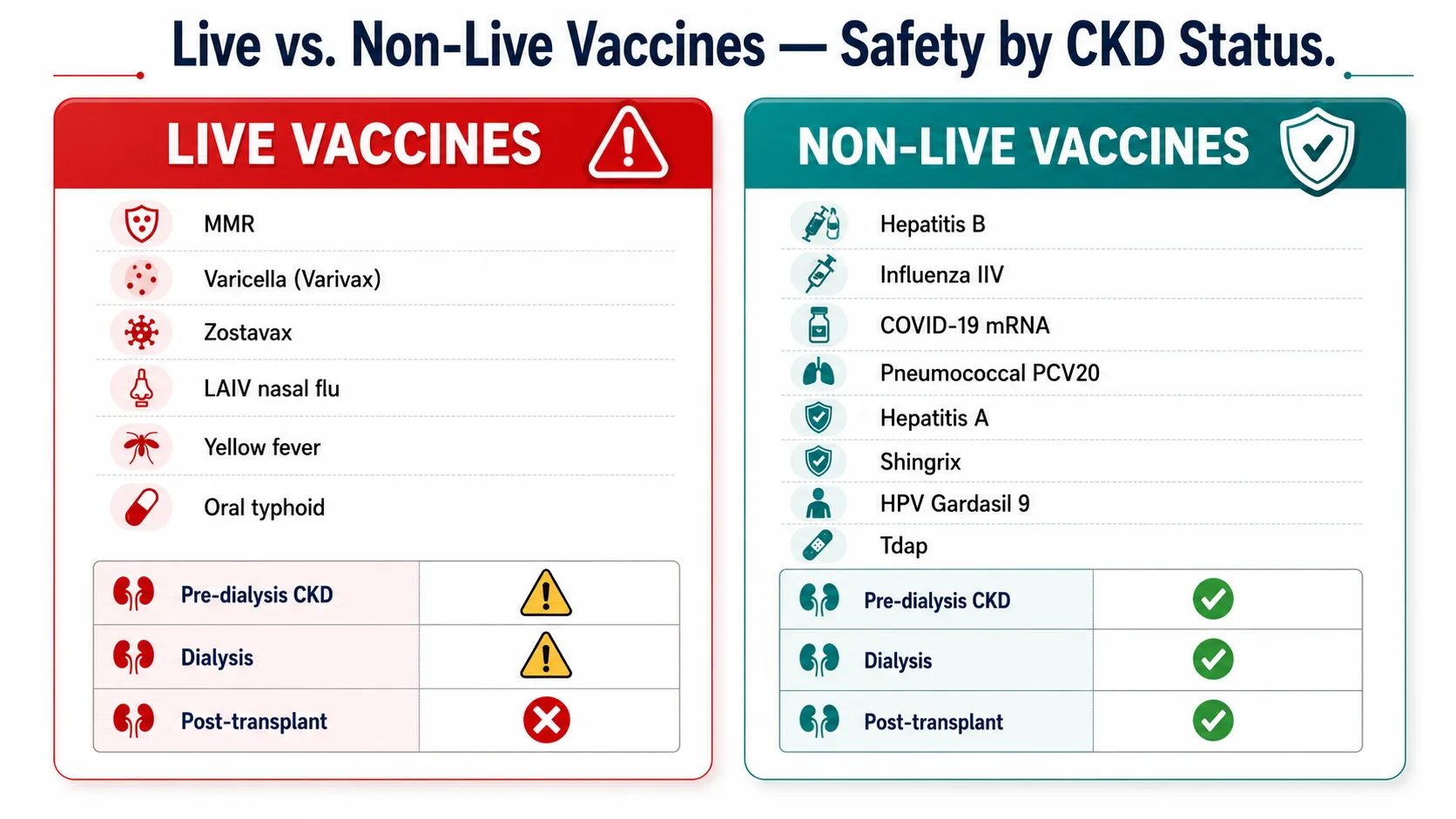
Fig. 2 — Live vs non-live vaccines in CKD: non-live (inactivated) vaccines are safe at all CKD stages including post-transplant. Live attenuated vaccines (MMR, varicella, zoster Zostavax) should be given BEFORE transplant — they are contraindicated after immunosuppression starts because the live viral component can cause disease in an immunocompromised host. Recombinant or adjuvanted alternatives exist for most live vaccines: Shingrix (RZV) replaces Zostavax; IXIARO replaces the older live JEV vaccine.
| For educational use only · Not a substitute for individualized medical advice · williamriveromd.com |
williamriveromd.com
Page 3 |
| Viral Infections & Vaccinations Guide for CKD · williamriveromd.com |
W.G.M. Rivero MD · FPCP · DPSN · williamriveromd.com · 2026 |
Pre-Transplant Vaccination Checklist
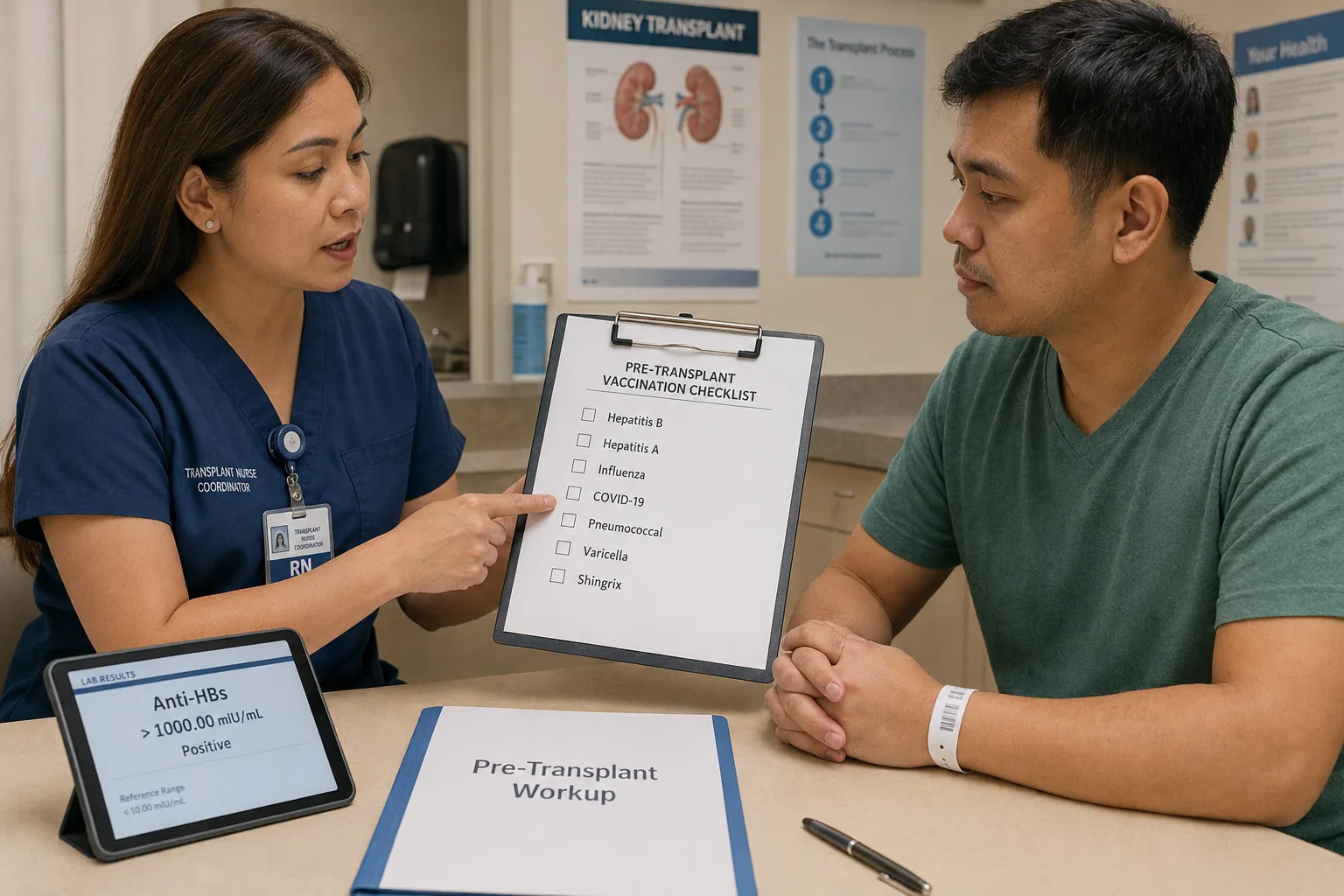
Fig. 3 — Pre-transplant vaccination checklist: all live vaccines must be completed ≥4 weeks before immunosuppression starts. Hepatitis B, COVID-19, influenza, pneumococcal, HAV, Shingrix, MMR (if needed), and varicella (if non-immune) should be reviewed at every CKD 4–5 visit — don't wait until the transplant listing date. Once immunosuppression begins, live vaccines are permanently contraindicated for as long as the patient remains on anti-rejection medications.
| For educational use only · Not a substitute for individualized medical advice · williamriveromd.com |
williamriveromd.com
Page 5 |
Key Viral Infections in CKD · Household Protection Prevention, recognition, and when to seek help |
Page 6 · williamriveromd.com |
Key Infections to Watch For
🔵 Influenza
Sudden high fever, severe muscle aches, and extreme fatigue. CKD patients are at risk of acute kidney injury on CKD from dehydration and the direct viral effect on tubular cells. Annual inactivated flu vaccine is mandatory. If symptoms begin: start oseltamivir (Tamiflu) within 48 hours — do not wait for test results. Call your nephrologist.
|
🔵 COVID-19
CKD and dialysis patients have significantly higher COVID-19 mortality compared to the general population. Follow the high-dose vaccination schedule (extra doses for dialysis patients). Early antiviral therapy with Paxlovid (nirmatrelvir/ritonavir) is effective — but check drug interactions with immunosuppressants (tacrolimus levels can spike). Report to your nephrologist at first symptoms.
|
🔴 Hepatitis B
May be completely asymptomatic for years — detected only on blood tests. Transmitted via HD equipment, blood transfusions, tattooing, and unprotected sex. Mandatory anti-HBs titer check every 6 months for all HD patients. If HBsAg becomes positive, patient must be isolated to a dedicated HBsAg+ dialysis station immediately. Annual liver ultrasound for chronically infected patients.
|
🟡 Herpes Zoster (Shingles)
Painful, blistering rash following a dermatomal distribution — one side of the body or face. CKD patients are at significantly higher risk due to T-cell dysfunction. Start acyclovir or valacyclovir within 72 hours of rash onset for best results. Dose-adjust for kidney function. Shingrix (RZV) vaccine significantly reduces both the incidence and severity of shingles — preferred over the older Zostavax live vaccine.
|
Household Cocooning — Protecting the CKD Patient by Vaccinating Everyone Around Them
Cocooning means protecting a vulnerable person by ensuring that everyone who lives with or cares for them is immunized — reducing the chance that an infectious disease enters the home. For CKD and dialysis patients in multi-generational Filipino households, cocooning is especially important.
- All household members: annual inactivated flu vaccine — the single most impactful cocooning measure
- Children in the household: ensure MMR, varicella, and COVID-19 vaccine schedules are complete and up to date
- Household members with active cold or flu: wear a surgical mask at home and maintain distance from the CKD patient
- No sharing of food utensils, drinking glasses, toothbrushes, or razors with dialysis patients
- Visitors with active respiratory illness: politely ask them to reschedule their visit until they recover
- Caregivers: wash hands with soap and water for at least 20 seconds before assisting with dialysis-related care
Dialysis Unit Infection Control — Know Your Rights
Separate Area for HBsAg+ Patients
DOH and KDIGO standards require that Hepatitis B surface antigen-positive patients be dialyzed in a physically separate area with dedicated machines. Ask your dialysis unit if this standard is being met.
|
Dedicated Staff for HBsAg+ Section
Staff caring for HBsAg+ patients should not simultaneously care for HBsAg-negative patients during the same session. Cross-contamination via gloves, equipment, and multi-dose vials is a known transmission route.
|
Report Symptoms SAME DAY
Report any jaundice (yellowing of eyes or skin), unexplained fatigue, dark urine, or fever during or after a dialysis session to the dialysis nurse on the same day. Do not wait for the next session.
|
| KDIGO 2024 · PSMID Immunization Guidelines 2024 · DOH Philippines · Educational use only. |
williamriveromd.com · Page 6 of 9 |
| Viral Infections & Vaccinations Guide for CKD · williamriveromd.com |
W.G.M. Rivero MD · FPCP · DPSN · williamriveromd.com · 2026 |
Household Cocooning — Philippines Context

Fig. 4 — Household cocooning in the Philippine context: when a CKD or dialysis patient lives in a multi-generational household (the norm in the Philippines), vaccinating all household members reduces the patient's exposure risk significantly. Annual influenza vaccination for all family members is the single most impactful cocooning measure. Ensuring that children's MMR, varicella, and COVID-19 schedules are complete removes additional household transmission risks that can be particularly dangerous for immunocompromised patients.
| For educational use only · Not a substitute for individualized medical advice · williamriveromd.com |
williamriveromd.com
Page 7 |
| Viral Infections & Vaccinations Guide for CKD · williamriveromd.com |
W.G.M. Rivero MD · FPCP · DPSN · williamriveromd.com · 2026 |
Dialysis Unit Coinfection Protocol
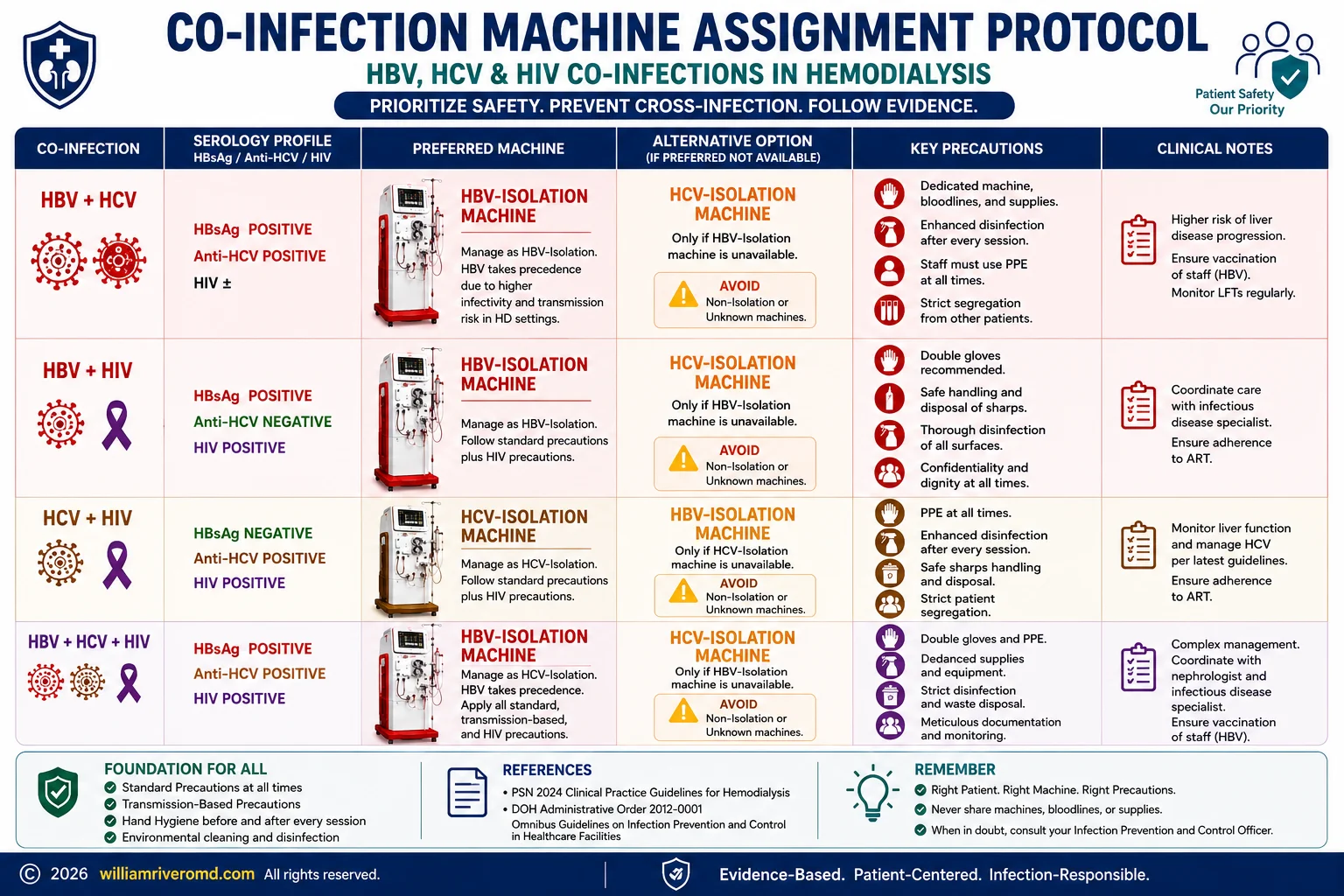
Fig. 5 — Dialysis unit coinfection protocol: isolation procedures for Hepatitis B-positive patients, machine decontamination standards, and the reporting chain when a patient develops fever or jaundice during a dialysis session. Patients have the right to ask their dialysis center about their infection control practices. An HBsAg-positive patient who is not being dialyzed in a separate dedicated area is being exposed to a preventable risk — report concerns to your nephrologist or the DOH.
| For educational use only · Not a substitute for individualized medical advice · williamriveromd.com |
williamriveromd.com
Page 8 |
When to Seek Help · Travel Vaccines · Quick Reference Emergency signs · Travel vaccination for CKD · Safe vs. contraindicated vaccine list |
Page 9 · williamriveromd.com |
🚨 Go to the ER Immediately If You Have Any of These
- Fever >38.5°C with shaking chills — possible sepsis from vascular access or pneumonia
- Cough + shortness of breath that develops rapidly — possible COVID-19 or bacterial pneumonia
- Jaundice (yellowing of skin or eyes) + dark urine — possible acute hepatitis
- Decreased urine output during an illness — AKI on CKD requiring urgent assessment
- Confusion, extreme weakness, or inability to stand — possible septic encephalopathy
Travel Vaccination Considerations for CKD Patients
| Destination |
Required / Recommended Vaccine |
CKD Notes |
| Domestic Philippines | Typhoid (Vi polysaccharide), Hepatitis A | Safe — both non-live; Vi polysaccharide typhoid is preferred over oral Ty21a (live) |
| Southeast Asia | Japanese Encephalitis (JEV) | Inactivated IXIARO — safe for all CKD stages including post-transplant |
| Africa / South America | Yellow Fever | LIVE — avoid if immunosuppressed; obtain medical exemption certificate from travel medicine clinic |
| Meningococcal belt (Hajj, Sub-Saharan Africa) | Meningococcal ACWY | Safe — non-live conjugate vaccine; no dose adjustment needed |
⚠ Yellow Fever — LIVE Vaccine Alert
Yellow fever vaccine is a live attenuated vaccine — it is contraindicated in post-transplant patients and in anyone on significant immunosuppression. If travel to yellow fever-endemic areas is required, obtain a medical exemption certificate from an accredited travel medicine clinic. Some countries accept the exemption in lieu of proof of vaccination.
Quick Reference — Safe vs. Contraindicated Vaccines
✅ Non-Live Vaccines — SAFE at All CKD Stages Including Post-Transplant
Hepatitis B (higher dose required in CKD 4–5 and HD)
Influenza (IIV) — inactivated only; annual
Pneumococcal (PCV15, PCV20, PPSV23)
COVID-19 (mRNA or protein subunit)
Hepatitis A
Shingrix (RZV) — recombinant zoster vaccine
HPV (Cervarix or Gardasil-9)
Tdap / Td
Meningococcal ACWY
JEV (IXIARO) — inactivated Japanese encephalitis
Typhoid Vi polysaccharide (injection form)
|
🚫 Live Vaccines — Give BEFORE Transplant Only · CONTRAINDICATED After Immunosuppression
MMR (measles, mumps, rubella)
Varicella (VZV) — chickenpox vaccine
Zostavax — live zoster vaccine (use Shingrix instead)
Yellow Fever (YF-Vax)
LAIV — live attenuated influenza (nasal spray)
Oral typhoid Ty21a — capsule form
All live vaccines must be completed ≥4 weeks before starting immunosuppressive therapy. Once transplanted, they are permanently contraindicated while the patient is on anti-rejection medications.
|
Hepatitis B Screening at HD Transfer
When transferring to a new dialysis center, always bring your hepatitis B serology records (HBsAg, anti-HBs, anti-HBc) and your most recent anti-HBs titer. New centers must verify your serological status before placing you in a HD bay. This protects both you and other patients.
| Reference: PSMID Immunization Guidelines 2024 · PSN Guidelines · KDIGO 2024 · For educational use only · Confirm all vaccines with your nephrologist · williamriveromd.com · 2026 |
williamriveromd.com
Page 9 of 9 |