| 🔴 VERY HIGH PURINES (>200 mg/100g) — Avoid completely during flare; severely limit at all times |
| Dilis — dried anchovies | 600 mg | Extremely concentrated purines in dried form. A small handful delivers a massive uric acid load. Avoid entirely in gout. |
| Sardinas sa mantika — canned sardines in oil | 480 mg | Very high purines from fish flesh and canning liquid. Avoid during flares; limit to once per week at most otherwise. |
| Atay ng baboy / manok — pork / chicken liver | 444 mg | Highest purine load of any common Filipino food. Avoid completely — even 50g significantly raises serum UA. |
| Bato — kidney (pork / beef) | 325 mg | Organ meat — extremely high purines. Avoid completely. Common in goto, pares, and some kare-kare preparations. |
| Utak — brain (pork) | 250 mg | Very high purines. Avoid completely. Used in some sisig and kare-kare recipes. |
| Pusit — squid | 200 mg | High purines. Avoid during flares. Limit to small portions (≤50g) on non-flare days, infrequently. |
| Chicken / beef broth cubes (Knorr, Maggi) | Very high | Highly concentrated meat extracts — among the highest purine sources per gram. Use pandan or tanglad (lemongrass) for flavor instead. |
| 🟡 MODERATE PURINES (50–200 mg/100g) — Limit to 1 serving per day; avoid entirely during active flare |
| Manok — chicken breast/thigh (100g) | 175 mg | Moderate purines. One palm-sized piece (100g) per day is acceptable. Avoid skin. Boiled or grilled is preferred over fried. |
| Alimango / alimasag — crab (100g) | 152 mg | Moderate-high. Limit to ≤50g during non-flare periods. Avoid entirely during flares. |
| Hipon — shrimp (100g) | 150 mg | Limit to small portions (50g) occasionally. Higher purine than freshwater fish. |
| Baboy — pork (100g lean) | 150 mg | Limit to 1 serving/day. Avoid fatty cuts (liempo). Isaw (intestine) = organ = very high purines — avoid. |
| Baka — beef (100g lean) | 120 mg | 1 serving/day acceptable. Avoid beef broth (concentrated purines). Avoid bulalo (bone marrow). |
| Bangus — milkfish (100g) | 90 mg | Lower than many fish. One of the best fish choices for gout patients in the Philippines. 1 serving/day acceptable. |
| Tilapia (100g) | 80 mg | Reasonable purine level. 1 piece/day acceptable. Grilled or steamed preferred. |
| Kabute — mushroom (1 cup) | 60 mg | Plant purines — less readily absorbed than animal purines. Limit to 1 cup/day; avoid during active flare. |
| Monggo — mung beans (½ cup cooked) | 50 mg | Plant purines have minimal UA effect. Do NOT eliminate monggo for gout — large studies show legumes do not significantly raise serum UA. Excellent fiber and protein source. |
| Kangkong (1 cup cooked) | 40 mg | Very low actual risk despite being a moderate purine food. Eating kangkong does not significantly raise serum UA — safe daily vegetable. |
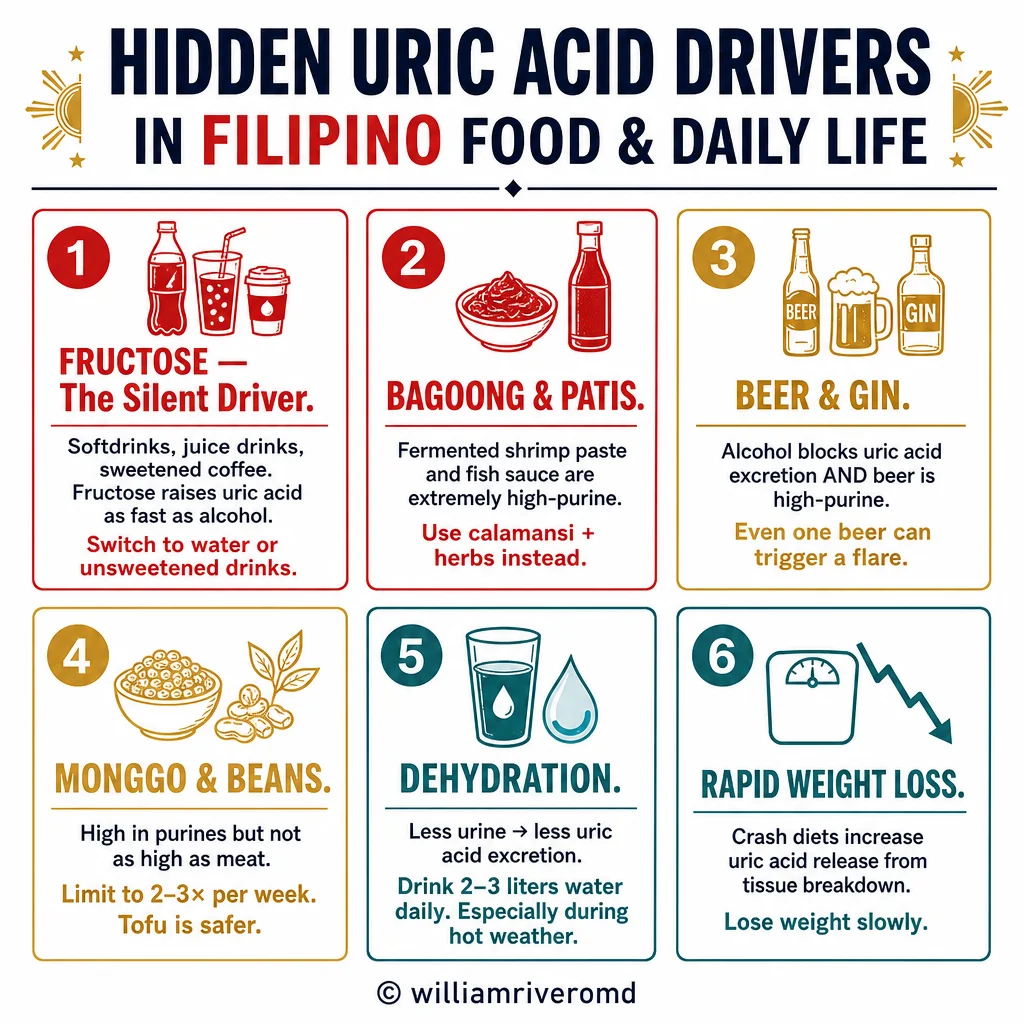
| Beer — 1 bottle (330 mL) | ★ Multiple | Single most potent gout trigger: raises UA via (1) guanosine content, (2) ethanol → accelerated purine breakdown, (3) lactic acid → impaired renal UA excretion. AVOID completely in gout. |
| 🟢 LOW PURINES — Safe choices; eat freely (in appropriate portions for other dietary restrictions) |
| Itlog — eggs (chicken or duck) | <1 mg | Essentially zero purines. Excellent protein source for gout patients. No restriction needed. |
| Gatas — low-fat milk, yogurt | <5 mg | Low-fat dairy may actively lower serum uric acid by promoting renal UA excretion. 1–2 glasses/day beneficial (check phosphorus in CKD). |
| Kanin / bigas — white rice | <5 mg | Lowest purine of any staple. Safe for gout. Preferred over brown rice in CKD 4–5 (lower phosphorus). |
| Kamote, cassava, saging saba (as starch) | <10 mg | Low purine starchy foods — safe for gout. Saba banana: check potassium if fluid-restricted. |
| Most fruits (pakwan, papaya, mangga, pinya) | <15 mg | Safe. Exception: avoid sweetened fruit juices and sodas — fructose raises serum UA independently of purines. |
| Tofu — white / silken | Moderate plant | Despite moderate plant purines, tofu does NOT raise serum UA in clinical studies — may be mildly protective. Safe to eat daily. |
| Kape — coffee (1–2 cups/day) | — | Coffee (regular or decaf) lowers serum uric acid and reduces gout risk in epidemiological studies. 1–2 cups/day may be beneficial. |
| Seresa — cherries (½ cup daily) | <5 mg | Cherry consumption associated with 35% lower gout flare risk. Anthocyanins inhibit xanthine oxidase and have anti-inflammatory effects. |